
by Darrel Crain, DC – ICPA.org: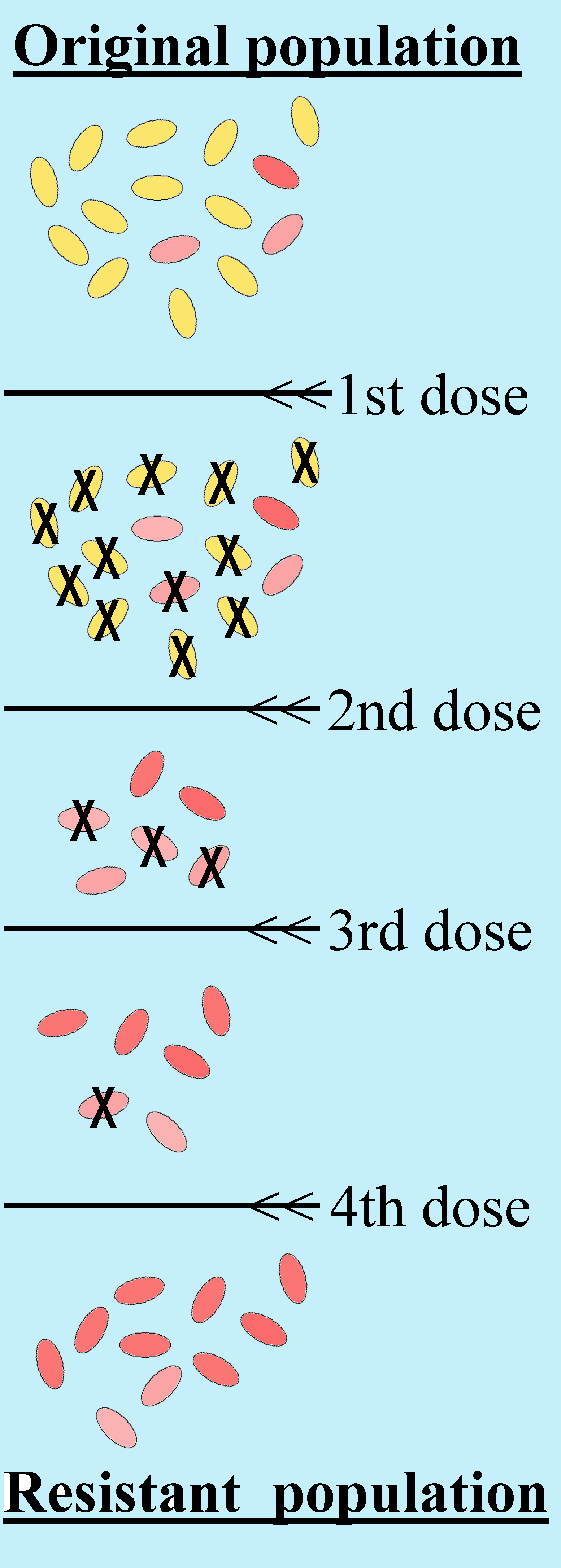
Earaches bring more unhappy children to emergency rooms and pediatric offices each year than just about any other health disorder. Antibiotics remain the most popular medical treatment for earache, with doctors reportedly writing 15 million prescriptions per year in the United States alone. It is estimated that at least half of the prescriptions are unnecessary and ineffective for helping this problem.
Due to the widespread overuse of antibiotics, drug-resistant germs have been reproducing as fast as frolicking rabbits, constantly evolving new levels of drug resistance. For over a decade our health leaders have been sounding the alarm to doctors to stop writing so many prescriptions for antibiotics because of growing drug resistance as well as serious health risks to the user.
“The risks of antibiotics, including gastrointestinal symptoms, allergic reactions, and accelerated resistance to bacterial pathogens must be weighed against their benefits for an illness that, for the most part, is self-limited,” according to the authors of a study about earache published in the Journal of the American Medical Association (JAMA) in September 2006.
Antibiotics are weapons of mass destruction intended to assassinate select gangs of bad-boy bacteria. Unfortunately, most of the hardworking, honest bacteria in the body get murdered at the same time, wiping out the body’s mighty microbes that normally do important work such as digesting food and making vitamins.
The earache study published in JAMA was a test of something called the “wait-and-see prescription” to help kids with earaches. This method has apparently been tried previously, but never before in an emergency room.
Half of the 283 children in the study diagnosed with acute otitis media (AOM) were sent home with a standard prescription, the other half with the wait-and-see prescription (WASP). The only difference between the two groups was that the parents in the WASP group were told to wait at least 48 hours before filling the antibiotic prescription.
“Everything comes if a man will only wait,” Benjamin Disraeli pointed out more than 150 years ago.
An unbelievable two out of three children avoided antibiotics with this innovative wait and- see strategy. “The WASP approach substantially reduced unnecessary use of antibiotics in children with AOM seen in an emergency department and may be an alternative to routine use of antimicrobials for treatment of such children,” according to the study.
The WASP concept may well be one of the greatest advances in medical science since the discovery of hand washing. The immediate benefit will be in the fight against two very pressing medical problems, microbial drug resistance caused by widespread antibiotic use, and antibiotic-induced chronic disease. But I can imagine applications throughout the medical profession. How about “wait-and-see surgery” for example?
The WASP study is sure to be criticized because it was only an observational study, not a clinical randomized trial (CRT). The CRT is considered the gold standard in medical science, so if the only thing you have is observational and anecdotal evidence to support your clinical practice, you might as well just use the paper to line your birdcage.
Which brings us to children who visit the chiropractor’s office for their earaches… Critics of chiropractic complain that there just isn’t any science to verify the ability of the chiropractic adjustment to enhance natural healing of the ears. The fact is, a significant number of studies have been published that describe the neurology and verify the benefits of chiropractic care for children, but alas, no clinical randomized trials.
And that reminds me of the famous parachute study, published in the British Medical Journal in December of 2003. The authors of this study write, “parachutes are widely used to prevent death and major injury after gravitational challenge,” yet the placebo-controlled, randomized clinical trials have never been done. I’m thinking that at this point it may be difficult to find people willing to jump from an airplane wearing a placebo parachute. It looks and feels like the real thing when you put it on, but when you pull the cord nothing happens.
“The perception that parachutes are a successful intervention is based largely on anecdotal evidence… As with many interventions intended to prevent ill health, the effectiveness of parachutes has not been subjected to rigorous evaluation by using randomized controlled trials,” write the authors.
Now I may be wrong, but it seems to me that people seeking good health are mostly interested in getting well as quickly as they can with having to worry about additional health risks. The wait-and-see prescription is not a recommendation to just ignore health problems and hope they go away, it is simply more evidence that the watchword for medical interventions is “less is more.”
Common sense suggests that if you need to jump out of a plane while still up in the air, you might want to strap on a real parachute without waiting for the double blind studies. I agree with the authors of the JAMA study who conclude, “Individuals who insist that all interventions need to be validated by a randomized controlled trial need to come down to earth with a bump.”
Article originally posted at ICPA.org.